Temporomandibular Joint / Jaw Pain (TMJ):
Chiropractic assessment:
Jessica is a 28 year-old administration manager that presented with recurrent problems with her jaw. Jessica described how her jaw problems have arisen without an obvious cause though she is in no doubt feels it is related to her stress at work. Over the past three months, Jessica has suffered from daily tension in her jaw and face, headaches and a click on the right side of her jaw. When at worst, Jessica’s symptoms include a ‘full feeling’ in the ears, headaches at the back and the front of her head.
Jessica does 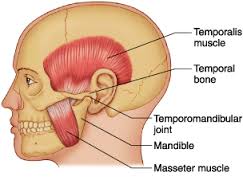 report that she grinds her teeth each night and more intensely when stressed by work but does deny clenching her teeth at work (though sometimes her staff make her feel that she should). To add to her woes, she has recently separated from her partner of five years and her father has been diagnosed with bowel cancer. Jessica wishes s
report that she grinds her teeth each night and more intensely when stressed by work but does deny clenching her teeth at work (though sometimes her staff make her feel that she should). To add to her woes, she has recently separated from her partner of five years and her father has been diagnosed with bowel cancer. Jessica wishes s
he was fitter and has difficulty fitting exercise into her demanding life. Work starts at 6.30 each morning and she rarely get home before 6 pm. Living on her own, and now carrying her mortgage without a second income adds strain to her predicament. Jessica denied a long-standing history of this problem and the only related condition she could recall was a significant whiplash injury 15 months ago.
Diagnosis:
When we examined Jessica, her posture showed that her head tilts to the right and she carries her head quite forward. While a facial scoliosis was absent, she is a Class II jaw occlusion with her lower jaw retracted. A degree of swelling was suspected below both eyes but no discolouration. Jessica’s upper back was also rounded, her muscles above the shoulder look overdeveloped and tense as does her muscles in front of her neck including the sternocleidomastiod muscle.
When asked to open her jaw fully, Jessica’s mouth opening was limited to 34 mm (6 less than normal) with a slight deviation to the left. A small palpable (but almost inaudible) click was also noted on opening on the right side. Tight irritable bands (myofascial trigger points) were felt in the muscles on both sides of the jaw, temples, below the jaw and the base of the skull and the back of the neck. These muscles produced symptoms similar to those described by Jessica. It was also possible to palpate such muscular finding on the intraoral muscles.
Jessica’s spinal movements were also compromised as she could not get her chin to reach her chest in normal posture and her ability to rotate her to the right and sidebend to the left was also limited. Furthermore, her upper back extension was quite reduced. On deeper palpation of her spine, a loss of normal motion between vertebra was noted at the base of the skull on the left, at C2/3 on the right and T3/4 on the right.
We presented Jessica with a summary of our understanding of her condition and a plan of management. We considered that Jessica’s jaw symptoms were chiefly myofascial (muscular) sources of pain arising from faulty mechanics of her jaw and neck. The dysfunction of her upper neck (vertebral subluxation) could not be ruled out as part of her altered head and neck mechanics and suboptimal neurological control. We suspected that her neck component had lingered since her car accident. What also appears to be a key factor in Jessica’s condition is how her body reacts to the work pressures and emotional challenges she is experiencing. It is our experience and that of other clinicians is that people will increase the tension around their jaw in such emotional states and can ‘brux’ or clench their teeth beyond normal levels. This has the effect of perpetuating and mechanical tension in the muscles of her jaw and the temporomandibular joints. Finally, Jessica’s headaches are in our opinion, a component of her overall problem and not separate. The headaches are consistent with the vertebral subluxation in her neck – both in terms of disturbed muscular function and altered neurological control. And, the headaches tie in with the excessive tension in the face.
Treatment:
Chiropractic adjustments to Jessica’s neck and jaw are indicated in a case such as Jessica and we will work to understand which chiropractic adjustive technique provides the best relief and most comfort and well as confirming the technical aspects of our approach. Given the spread and layers of Jessica’s myofascial trigger points, she will benefit from muscular releases and sedation of the trigger points. To reinforce the effect, Jessica will be taught exercises to further relax the key muscles.
There are facets of her case that suggest that Jessica may need a team approach to overcome her complaint. There is enough duration, frequency, spread of symptoms and extraneous factors that suggests her problem is somewhat complex. Jessica would probably benefit from utilising our in-house massage therapy. There are appears to be too many muscles and soft tissues involved to be address in a regular chiropractic treatment session. We suspect that a review by a dentist expert in temporomandibular disorders would be useful and can arrange an assessment with one of the experts we collaborate with. Finally, we are keeping our mind open to the notion that Jessica may need support from some counselling and training in meditation and relaxation by a psychologist.