Sciatica and ‘Pseudosciatica’:
Chiropractic assessment:
Tricia is a 49-year-old woman who works in an administration role that requires her to stand most of the day. Tricia’s first experience with lower back and leg pain was 12 years ago with the birth of her second child. Unfortunately her back and legs have troubled her ever since.
Tricia described her problems at length. During the birth she had an epidural injection and the birth itself generated tremendous low back pain. Tricia described pain at the base of her lower back that was intense in her left hip and spread to the outer font of the left thigh and into the calf. While the hip pain is strong and persistent, the symptoms were more of an ache in the lower limb.
These days Tricia says that her ‘hips annoy’ and make her feel more irritable and makes her feel ‘down’ and always weak on the left side, so much so that she ‘hobbles in the morning’ with left foot pain. While she is able to ‘keep up with’ her job, her back and lower limb condition drains her of the energy she wishes she could have to look after her family. Obviously Tricia has sought help for her problems by consulting her GP, a podiatrist and a naturopath. Her GP arranged for corticosteroid injections, the first one to the base of the lower back and a second one six months later to the iliotibial band (outer upper left thigh). In addition, the GP prescribed Ceramal (an antidepressant). Between the discussions of her GP regarding the results of her x-rays and CT scans, and her own reading, Tricia understands that her problem is a result of a degenerated lumbar disc and degeneration in her left hip. She states her problem is sciatica and a bad hip.
What was clear in the story that Tricia told was that in addition to the length of time and the extent that she has suffered, she is very frustrated and her condition has a significant impact on the quality of life.
A brief analysis of Tricia’s gait was not particularly remarkable. A small degree of increased foot pronation occurs and a small amount of pelvis sway was also noted. The most obvious finding was how stiff her upper body is held when she walks. When examining Tricia’s posture some deficits were readily identified. Tricia’s pelvis is lower on the left and rotated to that side. She has flat feet and a little knock-kneed which is more pronounced on the left. Tricia’s left shoulder is also lower, she has a sway back (increased lumbar lordosis) and is rounded in the mid back (increased thoracic kyphosis). Unfortunately Tricia looks quite unfit; her Body Mass Index (BMI) is 34 so she is obese and looks that way with most of her weight gain in her hips and thighs in a classic pear shape. In fact, the lack of proper muscle tone is visible in her gluteal, feet and thigh muscles.
Looking at Tricia’s range of motion, she appears to be quite mobile by background but when she performs a multisegmental rotation (see diagram 1. on next page), a loss of range is observed in the pelvis especially on rotation to the right. A lesser degree of restriction is noted in the thoracic rotation. Tricia’s forward bending to touch her toes is nearly full but the extension of her thoracic spine was moderately limited. A single leg stance test was used to give insight to how well Tricia could balance on her feet: with her eyes open she was within normal range of 25 seconds on each foot but with her eyes closed, she was unable to balance for more than 3 or 4 seconds. At the same time, her pelvis would deviate more to each side than normal and more pronounced on the left. A single leg squat showed stability was compromised, as each knee would deviate towards the midline and again this was more noticeable on the left.
to give insight to how well Tricia could balance on her feet: with her eyes open she was within normal range of 25 seconds on each foot but with her eyes closed, she was unable to balance for more than 3 or 4 seconds. At the same time, her pelvis would deviate more to each side than normal and more pronounced on the left. A single leg squat showed stability was compromised, as each knee would deviate towards the midline and again this was more noticeable on the left.
Once sitting, evaluation of hip rotation was performed and external rotation was limited to 27 degrees on the left 30 on the right and internal rotation was limited to 20 degrees on the left and 32 right (see diagram 2.). Observing hip flexion while seated showed excessive trunk movement especially on the left. A seated Slump test was conducted and this did not show any symptoms or limitations. Deep tendon reflexes were active, equal and normal.
While supine, orthopaedic tests of the hips were carried out without any significant findings. Abduction of both hips was moderately limited by muscle tightness and again this was more obvious on the left. Similarly, assessment of the length of other muscles was performed and the left iliotibial band on the outside of the thigh was noticeably tighter and shorter than normal.
The same was noted in left hip flexion but no pain was provoked. Straight leg raising tests were very unremarkable. Palpation of the hip and thigh musculature easily demonstrated tender taut muscles in the areas already described in this paragraph with myofascial trigger points (tight tender ‘knots’ in muscles that can radiate pain). These trigger points were particularly numerous and obvious around the left hip and outer thigh. Assessment of Tricia’s foot and ankle was performed at this time and her subtalar joint was stiffer and loss of normal motion was noted in dorsiflexion though not to the same degree as her hip and pelvis findings. While prone, assessment of the gluteal muscles and the foot was double-checked. In fact, the lack of healthy tone commented on previously was confirmed. When asked to lift her whole lower limb from the table, it was easy to see Tricia’s low back curve increase and the lack of control she has in her pelvis. Springing and palpating the sacroiliac joints showed distinct loss of normal motion on the left with concomitant tenderness in the surrounding ligaments. Similar loss of normal joint motion was noted in the mid-thoracic spine and upper cervical spine especially on the left. Reviewing Tricia’s radiological imaging showed a body that was within normal changes for her age and state of health. The scans did not suggest that a particular segment was at fault and similarly her hip findings were so mild they could be dismissed
as the main culprit.
 All these findings were discussed with Tricia. She was surprised that we did not believe she suffers from sciatica at all nor does she have a lumbar disc problem. To add to the contradiction, we disagreed that Tricia suffers from a primary hip disorder. We felt that there were a number of dysfunctions in her pelvis though. We suggested that her left sacroiliac joint was a key dysfunctional factor that we could assist via chiropractic adjustments.
All these findings were discussed with Tricia. She was surprised that we did not believe she suffers from sciatica at all nor does she have a lumbar disc problem. To add to the contradiction, we disagreed that Tricia suffers from a primary hip disorder. We felt that there were a number of dysfunctions in her pelvis though. We suggested that her left sacroiliac joint was a key dysfunctional factor that we could assist via chiropractic adjustments.
The plan from our point of view was to build greater confidence and independence in Tricia’s health and wellbeing by re-framing and educating her about what we felt to be ill-fitting previous diagnoses and the over emphasis on structural pathology. It appeared to us that she had previously had a lack of reassurance of her concerns on the perceived degeneration and pathology. An area that was flagged for later investigation was to consider a hormonal influence in her condition and strategies to manage this in collaboration with her GP or other health care providers.
Tricia was treated with a series of chiropractic adjustments to her sacroiliac joint and thoracic spine, mobilisation and stretching of her hip; PNF style stretching of her tight muscles. This was supported by training Tricia in a program of exercises to stretch the particularly tight tissues and to devlop better muscular (motor) control of her core trunk muscles, gluteals and foot muscles. While Tricia appeared to respond favorably, the long term prognosis remained a concern. She was therefore referrred for a podiattric consultation and assessment. Furthermore, given the large number of muscular and soft tissue issues, massage therapy was suggested to acclerate her progress in the short-term and to assist supporting Tricia in the long-term.
2. Hip internal rotation
1. Multisegmental rotation
Podiatry approach:
Tricia was then referred from our Chiropractor for assessment of her gait and lower limb function. Her primary symptom that led to her Chiro appointment was lower back pain but following their assessment, further symptoms/problems became apparent. The results of the chiropractic assessment relevant to her Podiatry appointment were:
• History of lower back and leg pain starting 12 years ago following the birth of her second child.
• Previous assessment by a Podiatrist only resulted in basic footwear advice to help with her “flat feet.”
• Recent scans have showed degeneration of her left hip joint.
• Basic gait assessment showed abnormal pronation (rolling in) and minor pelvic sway.
• The pelvis is lower on left side (as was her left shoulder) as well as genu valgum (knock knees) more obvious on left leg.
• Reduced hip range of motion (ROM) on left side compared to right as well as simliar tightness of the outer thigh (ITB) in left leg/thigh.
• Stiffness in sub-talar joint of the ankle (STJ) and limited dorsiflexion(flexing upwards) of both ankles.
Further questioning during her podiatry appointment also revealed a history of poor footwear habits, mainly thongs and slip on shoes and occasional plantar heel pain, which she describes as “spurs.”
Functional Assessment:
Quick visual assessment of stance showed similar features in hip and shoulder alignment as previously reported by Chiropractor. Both feet are pronated when weightbearing, with the left falling to 5 degrees everted in resting stance, compared to right that is only 3 degrees. Both are able to achieve 0 degrees when placed into the neutral stance (that
is, where the ankle and heel are perfectly aligned). When in the neutral stance position, the alignment of the knees and hips improves greatly.
Working Diagnosis:
With the left knee and foot pronating (rolling in) more than the right when standing (or weightbearing), it creates an acquired leg length difference, thus loading more pressure on the left hip joint. This is not solely the cause of her back pain but may be contributing to the poor results she has attained with previous treatments. Essentially, all the
good work done is undone as soon as she walked out the door. The excessive pronation is also overloading the muscles and ligaments in the arches of her feet, leading to a case of intermittent plantarfasciitis which causes her heel pain. Long term, strengthening exercises may help improve her function and lower limb posture, but improved, more supportive footwear, along with orthotics, will allow more even function across both legs and reduce the pelvis’ habit of overloading the left side. Further discussions with the Chiropractor may result in a small lift being placed under her left foot temporarily to improve the pelvic alignment.
Treatment:
Tricia’s main focus at the moment is to return to exercise in order to lose some weight. Subsequently, the footwear recommendations at the moment will be sports shoes. Joggers which are designed to support the inside of her foot are recommended, with all brands now carrying shoes for different foot types and functions. We discussed different orthotic options with Tricia. Preformed orthotics are a good option, being cheaper and quick to fit, but I have recommended a custom-made version for her due to the difference in function and posture between her left and right foot/leg. Custom-made orthotics are fabricated following a 3D scan of her feet and multiple measurements to work out exactly what each foot needs. They are more expensive in the short term but allow both the Podiatrist and the Chiropractor to incorporate different features to suit Tricia’s individual needs. They can also be adjusted and modified over a 3-4 year period as her needs change and hopefully fitness levels improve.
Massage Therapy:
Tricia, was referred to me by her chiropractor and podiatrist for some massage to assist in her treatment for lower back, hip and leg pain. Suffering discomfort for this extended period has affected Tricia’s quality of life so part of my focus will be on reducing her tension and alleviating any anxiety about her back, hip and leg, as well as treating the muscles at the core of her issues. Having been provided with a postural observation and gait analysis the ideal areas to address were highlighted. The presenting condition required work on the left more than right buttocks (gluteals), pelvis and hip musculature, with the front of the thigh and the calf as well as the muscles of the feet themselves. As for the other postural inadequacies, the neck and upper back required some attention. I began by releasing the hip flexors (deep in the abdomen) which allows for some reduction in pressure on the lumbar spine. While still on her back, I then released the muscles of the front neck to address the tension and upper back rounding. Next, I worked on the outer hip muscle to help reduce the overall tightness in the outer thigh, moving down through the quads and
into the outer knee.

While Tricia was side-lying, I used an elbow to release the trigger points in the muscles on the outside of the hip. From here I spent a short time working the tension from the adductors to even out the pressure on the hip and leg.
Moving onto the lower leg, I stretched and lengthened the calf before working deeply into the sole of the foot, in particular the arch. From here I worked on the back of Tricia’s lower legs, finding tension in all the muscle groups in the calf . The arches of the feet were particularly tight and tender. Some time was spent working deeper into the back of the pelvis and around the spot where the chiropractor thought that left sacroiliac joint has been generating discomfort. To further address the rounded upper back, I worked in though the spinal extensor and suboccipital
muscles at the base of the skull and the upper neck. Having released tension from the front of the neck earlier in the treatment, there was less force needed to penetrate into the tighter tissues causing that exaggerated round posture
and neck discomfort. After her treatment I recommended some stretches to target the hip muscles that seemed to
be most contributing to her discomfort, as well as a hip flexor stretch to help prevent the lower back from becoming so tight and sore. I also demonstrated a simple neck retraction exercise to help strengthen the deep neck flexors and reduce the frequency of upper back/shoulder tightness. Tricia reported a decrease in tightness and pain in her left lower back and hip and found movement less restricted after treatment.

Phil is 42 years old, married and has two young children. He has for the past 18 years worked at a desk job in journalism namely in the sports department, which in general incorporates long, long hours at the desk, eating his meals at the desk etc. Phil also plays touch football at a good level, of which he does twice weekly, this includes no holding back when playing.
Phil’s job is very stressful, with many deadlines. He complains of headaches, stiff neck and sore hips. He has visited his doctor who prescribed muscle relaxant tablets, which didn’t do much for him, just sent him to the toilet a lot. I initially explained that he needed to change his desk posture to a stand up desk, also, it was important to take breaks, even if it was just for lunch. I gave him a sheet of stand up stretches to do at this desk through the week.
Phil was attending the clinic on a weekly basis, concentrating on his neck and shoulders firstly. Using the trigger point technique, we were able to show him what he could achieve with regular treatment by him and myself together. The headaches and stiffness improved significantly over the coming weeks and then we started to look at his hip pain/soreness. His gluts were not firing, so again using trigger therapy, it allowed me to give him relief, although it never seemed to go away.
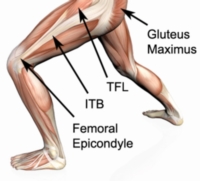
I introduced him to a foam roller and explained how to use it in the gluteal, (ITB) Illiotibial band, hip flexor and quad areas, all of which gave him great result, but again, it would return. After further conversation with Phil I found that during touch football he held nothing back and was “diving around like a teenage” his words. I referred him to a sports chiropractor who found that his hips were miss-aligned, further treatment with the chiropractor sorted out the hip problem and Phil now sees me on a regular basis for maintenance. He now stands at his desk and takes a regular lunch break.